A 44 year old male with pedal edema, SOB and decreased urine output.
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment
A 44 year old male, labourer by occupation, resident of nalgonda, came to OPD with chief complaints of swelling of both feet since 1 week, Shortness of breath since 3 days and decreased urine output since 3 days.
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 1 week ago and then he noticed pedal edema of both the feet which was insidious in onset, gradually progressive, extending upto ankle, pitting type, no aggravating factors and relieved on rest or by walking for a while. He also complained of shortness of breath Grade 2 (NYHA) which was insidious in onset, gradually progressive to Grade 3, no aggravating or relieving factors. There is no association of PND, orthopnea. It was also not associated with any chest palpitations, chest tightness. Patient also complained of decreased urine output since 3 days, insidious in onset, gradually progressive, hesitancy, pale yellow in colour. There is no history of fever, night sweats, cold, cough, nausea, vomiting, constipation, diarrhoea, pain etc.
PAST HISTORY:
There are no similar complaints seen in the past. Patient is a known case of hypertension since 11 years and is on telma. H. Patient is also a known case of diabetes since 11 years and is on metoclopromide. Patient is not a known case of TB, asthma, epilepsy, CAD, thyroid disorders.
FAMILY HISTORY:
There are no similar complaints in the family.
PERSONAL HISTORY:
Diet is mixed, appetite is decreased, sleep is adequate, bowel movements are regular, urine output is decreased, hesitancy. No known allergies. Non smoker and does not consume alcohol. Not any kind of medications
GENERAL EXAMINATION:
Patient is conscious, coherent and cooperative. Well oriented to time, place and person. Moderately built and moderately nourished.
There is bilateral pedal edema, pitting type, extending upto to ankle.There is no pallor, icterus, cyanosis, clubbing, lymphadenopathy.
Vitals --- BP: 150/80 mmHg PR: 84 bpm Temp: afebrile RR: 22 cpm
SYSTEMIC EXAMINATION:
Per abdomen:
On Inspection, shape of abdomen is flat, flank fullness is not present. No scars, sinuses, hernial orifices, dilated veins, visible pulsations. Umbilicus is centrally placed, inverted. No pigmentation.
On Palpation, all inspectory findings are confirmed. No local rise of tenderness. NO tenderness. Liver and spleen are not palpable.
On Percussion, no fluid thrill or shifitng dullness.
On Auscultation, bowel sounds are heard.
CVS: S1S2 heard; no murmurs heard
Resp: NVBS + BAE +
CNS: NAD +

PROVISIONAL DIAGNOSIS:
CKD..?
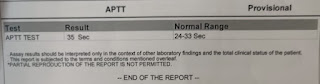
INVESTIGATIONS:









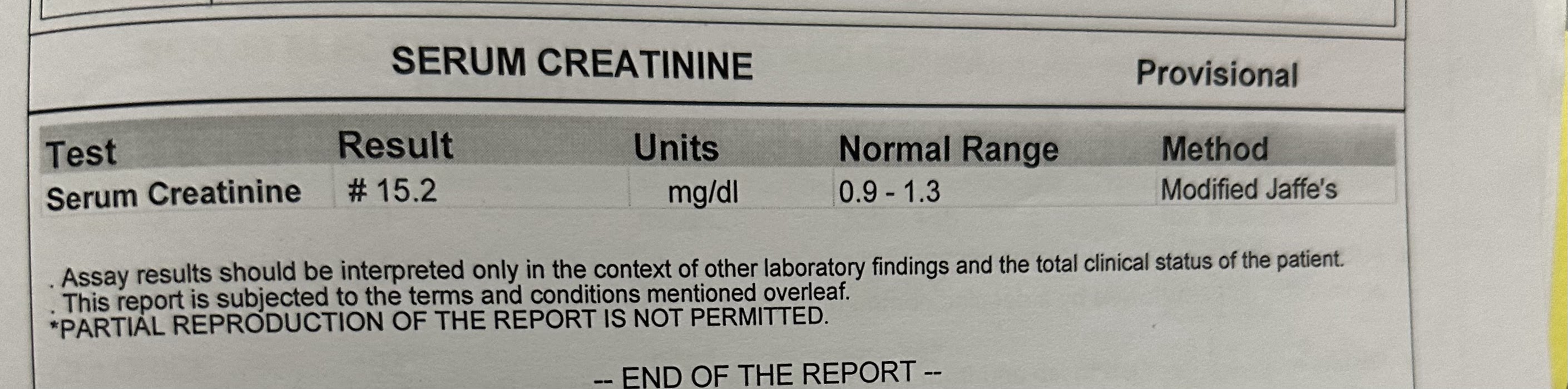



TREATMENT:
1. INJ.LASIX 40mg
2. TAB.NODOSIS 500mg PO/BD
3. INJ.PIPTAZ 4.5mg IV/STAT
4. INJ,PAN 40 mg IV/OD
5. TAB.NICARDIA 10mg PO/TID

Comments
Post a Comment