A 28 year old male with loss of appetite, hematuria and pedal edema.
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment
A 28 year old male, resident of Chityal, daily wage labourer by occupation, came to casualty with chief complaints of loss of appetite since 20 days, red coloured urine since 10 days and swelling of feet since 10 days.
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 20 days ago and then he had loss of appetite, insidious in onset, for which he went to hospital and got diagnosed as CLD, splenomegaly with portal hypertension and took medication. After which he developed red coloured urine since 10 days, insidious in onset, he also developed pedal edema, ptitting type extending upto ankle, aggravated on walking and relieved on taking rest. Patient has tremors since 15 days. No history of abdominal pain, vomitings, loose stool and burning micturition.
PAST HISTORY:
No similar complaints seen in the past. Patient is not a known case of Hypertension, diabetes, TB, thyroid disorders, epilepsy, CAD etc. No surgical history.
FAMILY HISTORY:
No similar complaints seen in the past.
PERSONAL HISTORY:
Diet is mixed, appetite decreased, sleep is not adequate, red coloured urine observed, bowel movements are regular. No known allergies. Chronic alcoholic since 6 years, increased his intake to 6 units everyday from 3 units. He is a non smoker.
GENERAL EXAMINATION:
Patient is conscious, coherent and cooperative. Well oriented to time place and person. Moderately built and moderately nourished. Pedal edema is present, non pitting type. No signs of pallor, icterus, cyanosis, clubbing, lymphadenopathy.
Vitals --- BP: 100/60 mmHg PR: 90 bpm Temp: afebrile (97.6 F) RR: 18 cpm
SYSTEMIC EXAMINATION:
CVS: S1, S2 heard, no murmurs, thrills, heave.
Resp: NVBS + BAE +
P/A: Soft, non tender, liver and spleen not palpable.
CNS: NAD+
PROVISIONAL DIAGNOSIS:
Decompensated liver disease..? Hepatic encephalopathy..? Alcohol dependance syndrome...?
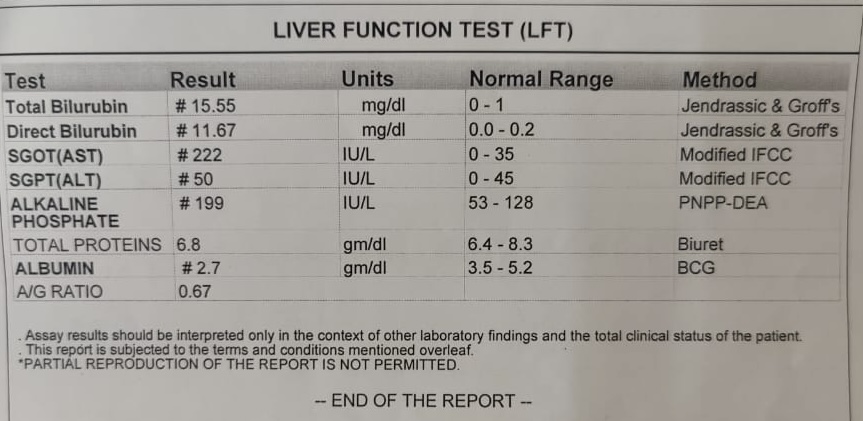
INVESTIGATIONS:










TREATMENT:
1. IV FLUIDS NS @ 75ml/hr
2. INJ. THIAMINE 200mg IV/BD
3. T.DOXY 100mg PO/BD
4. T.UDILIV 300mg PO/BD
5. T. OROFER xt PO/BD
6. T.OXAZEPAM 15mg

Comments
Post a Comment